
When Sleep Apnea Doesn’t Look Like Sleep Apnea
A Guide for the Wellness Focused Adult


This week’s post is a collaboration with Kat Fu, M.S. She is the founder of The Longevity Vault, where she writes about sleep, hormones, and longevity science for adults over 50. She holds dual master’s degrees - Biomechanics Engineering and Electrical Engineering - from Stanford University. Since 2007, she has applied an engineer’s analytical approach to health optimization, with her current focus being on helping individuals who struggle with middle-of-the-night wakeupe’s and shortened sleep. She writes at thelongevityvault.substack.com
If you picture someone with obstructive sleep apnea, the stereotype is familiar: a heavier middle-aged man, snoring loudly and nodding off at stoplights.
But there also exists a unique and increasingly prevalent phenotype.
Imagine a 52-year-old marathoner who wakes up feeling like he has a hangover without drinking, a 61-year-old executive whose bloodwork looks great but who lives with constant brain fog, and a 58-year-old teacher who eats well, walks every day, does “everything right”—and still feels like sleep never truly restores her.
They often say some version of:
“My study was ‘normal,’ but something is still wrong with my sleep.”
“My AHI is only 4, so they told me I don’t have sleep apnea.”
“I don’t even snore that much.”
The apnea–hypopnea index (AHI) is the number of times per hour of sleep that breathing stops completely (apnea) or partially collapses (hypopnea) for at least 10 seconds, usually with some drop in oxygen. In adults, an AHI under 5 events per hour is considered normal. AHI between 5 and 15 is labelled mild obstructive sleep apnea (OSA), 15–30 is moderate, and 30 or more is severe (Harvard Sleep Medicine).
AHI is useful, but it is not the whole story—especially for non-obese, midlife adults. This article walks through:
how sleep-disordered breathing can show up in people who are not overweight
how OSA shifts with age and stops looking “classic”
why a “normal” or “borderline” AHI doesn’t always match how you feel
how I think about treatment options once we stop treating you as just a number
When apnea doesn’t look dramatic
In leaner or older adults, sleep-disordered breathing often doesn’t present as dramatic gasping or daytime sleepiness.
More often, what I hear is about waking unrefreshed despite spending seven or eight hours in bed, or about a mental “battery” that drains too fast during the day. People describe slow thinking, word-finding problems, and a creeping loss of confidence in their memory. Mood shifts are common: more irritability, more anxiety, a sense of being “on edge” without a clear trigger.
Night-time often feels light and fragmented. You may wake many times without knowing why, or feel as if you never get into deep sleep even though your watch insists you’ve been in bed long enough. Daytime fatigue is real, but it’s less “falling asleep at red lights” and more “everything takes more effort than it should”.
All of this overlaps with other midlife themes—stress, perimenopause and menopause, caregiving load, work burnout—so it is easy to wave away. From the outside, these patients do not look like the textbook picture of sleep apnea. Many have a body mass index (BMI) in the normal or mildly elevated range. Some exercise regularly. Partners may notice occasional snoring or restless sleep, but nothing theatrical.
Non-obese OSA is common
For a long time, obesity was taught as the core risk factor for OSA. It certainly matters. But several large datasets have made something very clear: a substantial share of adults with OSA are not obese.
In a large community-based cohort of nearly 3,000 adults with OSA, the median BMI was just under 29, and about 60% had BMI below 30, meaning they were not in the obese range. A more recent individual-participant meta-analysis of over 12,000 adults found similar patterns: the majority of people with OSA were either overweight or of normal weight; only a minority had obesity.
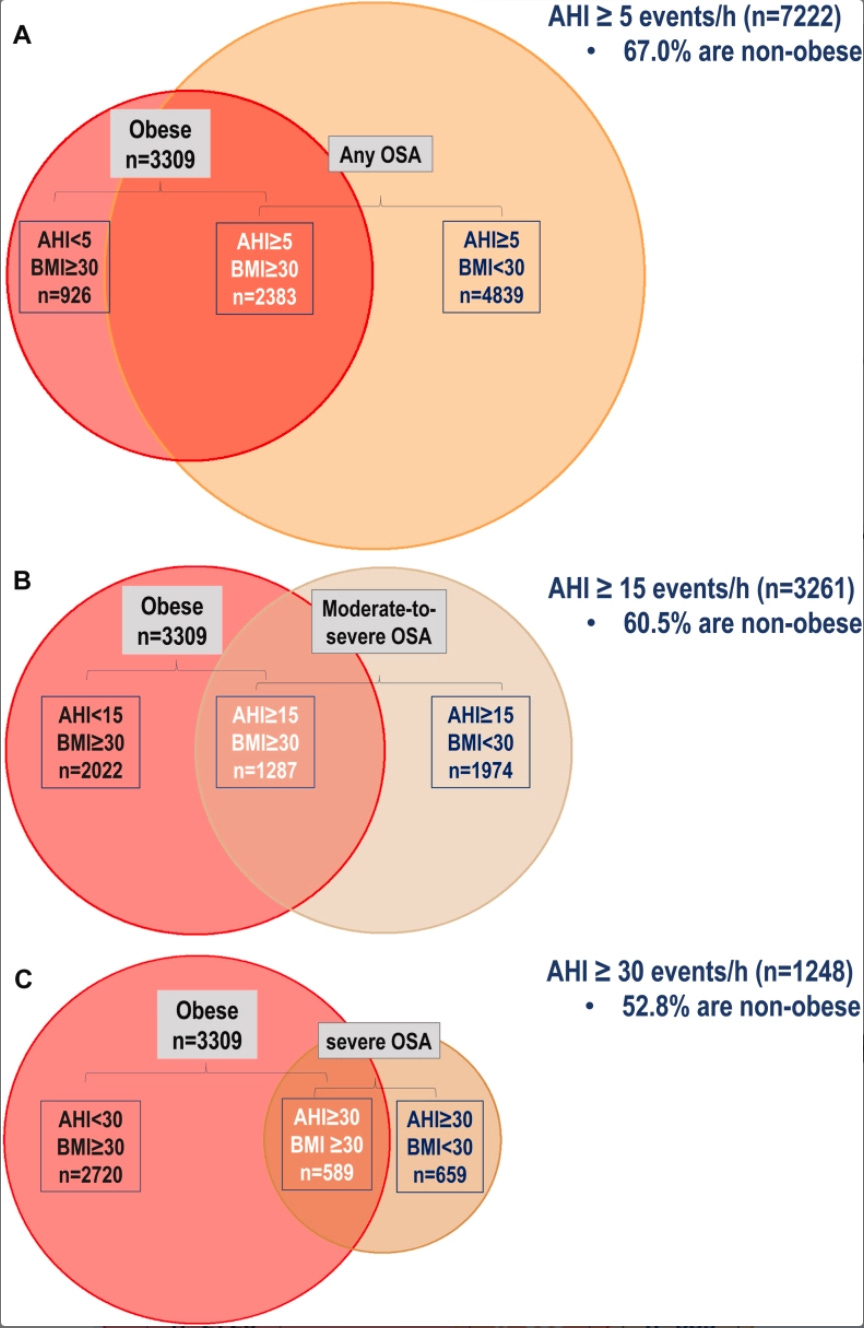
A. Intersection of obesity, defined by BMI ≥ 30 kg/m2 (red circle) and AHI ≥ 5 events/h (OSA). B. Intersection of obesity and AHI ≥ 15 events/h (moderate-to-severe OSA); C. Intersection of obesity and AHI ≥ 30 events/h (severe OSA). Percentage of individuals without obesity in each diagram is related to results of random-effects meta-analyses of prevalences. Esmaeili N, et al. The relationship between obesity and obstructive sleep apnea in four community-based cohorts: an individual participant data meta-analysis of 12,860 adults. EClinicalMedicine. 2025.
Another clinical series looked specifically at adults with OSA but no obesity. This group made up a substantial proportion of referrals. They tended to have different underlying drivers (for example, a very sensitive arousal threshold or airway shape issues rather than pure weight-related narrowing), and they were harder to treat with standard CPAP, with lower adherence.
The take-home is this:
You can be a fit, non-obese, health-conscious 55-year-old and still have sleep-disordered breathing that matters. Weight is just one risk factor.
How OSA changes with age: Obstructive sleep apnea is not one static disease
In younger, heavier adults, the airway problems are often driven by soft-tissue bulk and anatomy. The airway can collapse completely. You see large obstructive apneas, big drops in oxygen, loud snoring, and very obvious events on a sleep study.
In many older or non-obese adults, muscle tone decreases and control of breathing becomes more fragile. Rather than dramatic collapses, you see partial narrowing of the airway, with harder work of breathing, subtle restriction of airflow (often called flow limitation), and frequent brief awakenings as the brain keeps rescuing you. Oxygen levels may dip only slightly. On paper, the study can be described as “mild” or even “normal”, but subjectively, sleep feels broken.
This shift with age is one reason I listen carefully when a midlife patient says: “I don’t snore that badly, but I never feel like I get into deep sleep.” It doesn’t prove sleep-disordered breathing is present, but it keeps the door open to that possibility—even when BMI and laboratory tests look reassuring.
More on “OSA” representing many different phenotypes: Two people can have the same AHI and very different physiology.
Some patients have strongly anatomical disease: a smaller lower jaw, a crowded tongue space, or other structural narrowing that makes the airway prone to collapsing. Others have airways that are adequate on exam, but their brain’s control of breathing is highly sensitive (high “loop gain”), so small fluctuations in CO₂ lead to overshooting and undershooting of breathing. Some wake very easily with the slightest restriction in airflow (a low arousal threshold), while others sleep through far more marked events.
Events can also cluster
Some people have supine-predominant OSA, where breathing is much worse on their back, and much better on their side. Others have REM-predominant OSA, where events are concentrated in rapid eye movement sleep.
All of these variants can yield similar AHIs. An AHI of 8 in someone who snores loudly, feels fine, and has calm overnight oxygen traces is a different problem than an AHI of 8 in someone who is exhausted, foggy, and clearly distressed by their sleep. A single number does not capture that difference.
**Upper airway resistance syndrome (**UARS) and flow limitation
One pattern is sometimes labelled upper airway resistance syndrome (UARS). In UARS, the airway repeatedly narrows enough to make breathing harder and to trigger micro-arousals, but not enough to meet the standard scoring criteria for apnea or hypopnea. Oxygen levels usually stay near normal. AHI is often under 5, which puts you in the “no OSA” box by traditional rules.
Yet people with UARS frequently describe unrefreshing sleep, daytime fatigue, and “tired but wired” nights. In a study that compared patients with UARS to patients with mild OSA and to healthy controls, the UARS group actually reported worse sleep quality, more fatigue, and poorer early-morning attention than those with mild OSA, despite having a lower AHI.
Another related concept is flow limitation itself. Rather than looking only at events that meet the thresholds for apnea or hypopnea, you look at periods when airflow is clearly flattened or restricted, indicating that the upper airway is narrowed and breathing is more effortful.
Put simply:
You can have an AHI that looks reassuring on the report and still have enough disrupted breathing to leave you sleepy and impaired during the day.
When numbers and lived experience disagree
This is often where people feel unheard. They have done their homework. They have reduced caffeine, gone to bed more consistently, worked on their sleep environment, and tried to manage stress. They are doing the things any sensible clinician would advise.
They then have a sleep study which returns with an AHI of 2.8 or 4.3 and a comment like “no significant sleep apnea.” On paper, they are fine from health risk, but often they are symptomatically burdened.
In my practice, I talk about 3 pillars that guide whether we consider treatment:
Health risk. If the AHI and oxygen patterns clearly fall into a range known to increase cardiovascular and metabolic risk, that carries weight.
Impact on others. Loud snoring, gasping, or frequent awakenings can disrupt partners and family, and sometimes that alone motivates change.
Symptoms and function. If daytime performance, mood, and quality of life are meaningfully compromised, and other obvious causes have been addressed, that matters even when AHI is modest.
When all three point in the same direction, decisions are straightforward. When AHI looks “mild” or “borderline” but symptoms are severe, I am less interested in debating whether the label is OSA, UARS, or “just poor sleep,” and more interested in understanding the pattern and deciding whether targeted treatment might help.
The studies on non-obese OSA, UARS, and flow limitation are helpful here because they back up what patients have been saying for a long time: a single index can underestimate how disruptive their sleep-disordered breathing really is.
Beyond CPAP: a brief map of options
CPAP remains the standard treatment for moderate to severe OSA, and a trial can be useful even for people in the gray zones to see whether stabilizing breathing reduces symptoms. But it is not the sole option, especially for milder or phenotype-specific patterns.
For midlife patients, the conversation I have most often sounds like this:
“Your study doesn’t show severe obstruction, but you have a pattern that could be contributing to the way you feel. Let’s talk about what we can adjust and what we can support.”
Depending on anatomy, symptoms, and preferences, that might include:
1. Jaw-based and positional strategies
Mandibular advancement devices made by a qualified dentist, which gently move the lower jaw forward to widen the airway.
Positional therapy devices or methods, when events cluster almost entirely on the back and nearly vanish in side-sleeping positions.
2. Nasal and airway support
Addressing nasal obstruction with saline rinses, medicated sprays, or structural procedures when indicated.
Occasionally adding myofunctional (orofacial) therapy to improve muscle tone and tongue posture as an adjunct, not a stand-alone fix.
3. Whole-sleep context
Targeted insomnia treatment (often CBT-I) when difficulty falling asleep, staying asleep, or early wake-ups coexist with mild breathing disturbance.
Hormone support where appropriate (for example, perimenopause/menopause or testosterone changes that interact with stress tolerance, autonomic regulation, sleep quality, and airway stability).
Circadian alignment: consistent timing, morning light, and a stable anchor for the wake-time so the brain knows when deep sleep is supposed to happen.
Medication review to identify substances that worsen breathing stability or fragment sleep.
4. Potential surgical options
Surgical therapies for OSA broadly fall into several categories:
Nasal Surgery
Palatal Surgery
Tongue Base and Hypopharyngeal Surgery
Skeletal Surgery
Hypoglossal Nerve Stimulation
For someone who does not fit the classic snoring stereotype, we often end up combining a multitude of the above options. The goal is not to “treat an AHI,” it is to improve the person’s ability to wake up feeling like sleep did its job.
If you are in midlife and feel chronically unrefreshed, do not let a borderline-sounding report close the chapter.
Sleep-disordered breathing can present in many ways. AHI can underestimate the burden in people whose main problem is flow limitation and sleep fragmentation rather than dramatic apneas and desaturations. Phenotype work shows that different clusters of symptoms and traits behave differently and respond to different treatment mixes. Residual sleepiness research tells us that even when airway treatment is optimized, other contributors may still need to be addressed.
The practical takeaway:
Your lived experience matters as much as the line on the report.
Treatment conversations can and should extend past “CPAP or nothing,” especially in midlife adults who don’t fit the classic mold.
Listening carefully to symptoms, reading the sleep study for context, and using the full toolbox of airway and non-airway interventions is how we start to close the gap between “your numbers look fine” and “you feel like yourself again.”
—Chris Gouveia & Kat Fu
|
 | A guest post by
|
This is a very helpful article 🙏🏽. I’m a GP and eventually worked out myself that I probably had OSA. Because I was slim, healthy and fit, and Asian, I didn’t fit the stereotype, especially not 14 years ago, when there was less understanding than now. But I have a small jaw, congenitally missing teeth plus a lot of childhood orthodontics. My tongue shows the telltale ridging on all sides that shows it’s ‘too big’ for my jaw.
And fascinatingly, I was diagnosed with ADHD age 55 - research shows OSA is more prevalent in ADHD populations than the general population.
Anyhow, I use CPAP with good effect but my daughter didn’t tolerate it and uses a mandibular splint. Can’t blame her - CPAP isn’t a sexy look in your mid 20’s…
I am very grateful for the information you provide in your Substack. Keep up the good work. I am still in the problem solving phase of my OSA / poor sleep / insomnia / nocturnal hypoxia journey. It is a lifelong journey of self care and self awareness.